A bronchoscopy is an examination of the lungs carried out using a very fine endoscope. This is a thin tube that is passed through the nose, then down the windpipe into the lungs. Unlike an operation, there is no cutting involved so no scars. A bronchoscopy carried out when someone is awake would be quite unpleasant, so when children have a bronchoscopy, a general anaesthetic is used, so they are asleep throughout.
• The night before your bronchoscopy, food and fluid are restricted.
• Your child is not allowed anything to eat (this includes milk) for 6 hours before the procedure (a light meal is best before then).
• We start the bronchoscopy list at 2pm so nothing to eat after 7.30am.
• They are also not allowed anything to drink apart from clear fluid (water or diluted juice) up to 2 hours before the procedure, and then nothing after that. So last drink by 11.30am.
• If your child is breast fed, you can feed your child up to 4 hours before the procedure.
• The doctor will advise you of the approximate time of the procedure.
• Your doctor should tell you if you should take your medications with a little sip of water on the morning of the procedure.
• You need to come to the ward by 9am on the day.
A consultant anaesthetist will give the anaesthetic, usually assisted by another doctor (a specialist registrar). Your child may be able to choose whether to go to sleep by breathing anaesthetic gas from a mask over the face, or by having an injection. The final decision must be made by the consultant anaesthetist, who is responsible for the safety of your child whilst (s)he is asleep. You will have the opportunity to see a doctor from the anaesthetic team beforehand, when you can discuss what will happen. After the anaesthetic has been started and your child is asleep, a needle will be put into a vein so that other necessary drugs can be administered -this is called an intravenous drip. You are allowed to stay with your child in the anaesthetic room until (s)he is asleep, but be aware that many parents find it upsetting to see their child go to sleep like this
The bronchoscopy will then be done by a consultant paediatrician, usually with the assistance of another doctor, (again a specialist registrar) who may do part of the procedure, under the close supervision of the consultant. The bronchoscope is a very flexible tube, which is passed through the nose into the airway (the windpipe and tubes connected to the lung). Pictures from this are displayed on a screen, and a DVD recording is made, which can be referred to later if necessary. You and your child will be most welcome to see the DVD afterwards.
The bronchoscope is also be used to wash out the airways, using sterilised salty water, which is immediately sucked out again (bronchoalveolar lavage). This fluid is sent to the laboratory to check for infecting organisms and also to look at the types of inflammatory cells present.
We may also take tiny samples (about the size of a pinhead) from the surface of the inside of the airways (endobronchial biopsy). This is quite painless, though if your child coughs, there may be flecks of blood in the spit for a short time. These samples are sent to the laboratory to study the microscopic structure of the airway and to determine the types of inflammatory cells present.
We will, if possible, do anything else necessary which might be unpleasant or painful (such as taking blood samples) whilst your child is asleep. This will be explained to you separately, and your and your child’s consent sought in the normal way.
Please stay on the ward during the procedure in case something comes up and we need to speak to you straight away.
I will come and speak with you as soon as I can once the procedure is finished, and your child will be observed by a nurse. Tell the nurse if your child has any symptoms such as chest pain or difficulty breathing. The nurse will check the blood pressure, pulse, respiratory rate and oxygen saturation. Your child cannot eat or drink anything for 1-2 hours after the procedure because the throat may still be numb.
Many children stay overnight as other procedures are being carried out; I also get infants to stay as an extra precaution. However for those going home the same day, once your child has eaten and drunk and is comfortable, you will be able to leave, assuming the nurse is happy with the blood pressure etc.
If you are concerned about your child after you have gone home, you can always speak to a doctor. Please ring the hospital (0207 352 8121) and ask the operator to bleep the on-call paediatric respiratory registrar.
There are always small risks in having an anaesthetic, and the anaesthetist will explain these to you. There are also small risks in having a bronchoscopy. However, we perform more than 200 of these on children every year at this hospital, and the vast majority of these are without complications. The commonest reaction is a slightly high temperature, and normally paracetamol (Calpol) deals with this. Some children cough a bit more for the next 12-24 hours. We also caution parents of babies having the procedure in order to investigate stridor (noisy breathing due to difficulty breathing in) that they may need extra monitoring, or help with their breathing for a while afterwards. If necessary, they will be cared for in the paediatric intensive care unit, or high dependency unit and the anesthetist makes that decision at the end of the procedure.
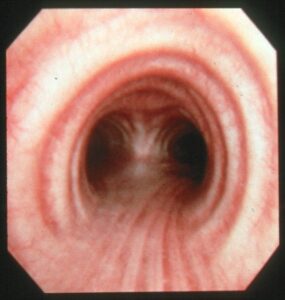
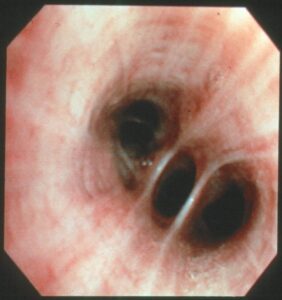
View looking through a bronchoscope. the picture on the left shows the trachea (windpipe) looking down to where it divides into the left and right main bronchi, which are the airways leading to the left and right lungs. The picture on the right is a view of the airways in the left lower lobe
A bronchoscopy is an examination of the lungs carried out using a very fine endoscope. This is a thin tube that is passed through the nose, then down the windpipe into the lungs. Unlike an operation, there is no cutting involved so no scars. A bronchoscopy carried out when someone is awake would be quite unpleasant, so when children have a bronchoscopy, a general anaesthetic is used, so they are asleep throughout.
• The night before your bronchoscopy, food and fluid are restricted.
• Your child is not allowed anything to eat (this includes milk) for 6 hours before the procedure (a light meal is best before then).
• We start the bronchoscopy list at 2pm so nothing to eat after 7.30am.
• They are also not allowed anything to drink apart from clear fluid (water or diluted juice) up to 2 hours before the procedure, and then nothing after that. So last drink by 11.30am.
• If your child is breast fed, you can feed your child up to 4 hours before the procedure.
• The doctor will advise you of the approximate time of the procedure.
• Your doctor should tell you if you should take your medications with a little sip of water on the morning of the procedure.
• You need to come to the ward by 9am on the day.
A consultant anaesthetist will give the anaesthetic, usually assisted by another doctor (a specialist registrar). Your child may be able to choose whether to go to sleep by breathing anaesthetic gas from a mask over the face, or by having an injection. The final decision must be made by the consultant anaesthetist, who is responsible for the safety of your child whilst (s)he is asleep. You will have the opportunity to see a doctor from the anaesthetic team beforehand, when you can discuss what will happen. After the anaesthetic has been started and your child is asleep, a needle will be put into a vein so that other necessary drugs can be administered -this is called an intravenous drip. You are allowed to stay with your child in the anaesthetic room until (s)he is asleep, but be aware that many parents find it upsetting to see their child go to sleep like this
The bronchoscopy will then be done by a consultant paediatrician, usually with the assistance of another doctor, (again a specialist registrar) who may do part of the procedure, under the close supervision of the consultant. The bronchoscope is a very flexible tube, which is passed through the nose into the airway (the windpipe and tubes connected to the lung). Pictures from this are displayed on a screen, and a DVD recording is made, which can be referred to later if necessary. You and your child will be most welcome to see the DVD afterwards.
The bronchoscope is also be used to wash out the airways, using sterilised salty water, which is immediately sucked out again (bronchoalveolar lavage). This fluid is sent to the laboratory to check for infecting organisms and also to look at the types of inflammatory cells present.
We may also take tiny samples (about the size of a pinhead) from the surface of the inside of the airways (endobronchial biopsy). This is quite painless, though if your child coughs, there may be flecks of blood in the spit for a short time. These samples are sent to the laboratory to study the microscopic structure of the airway and to determine the types of inflammatory cells present.
We will, if possible, do anything else necessary which might be unpleasant or painful (such as taking blood samples) whilst your child is asleep. This will be explained to you separately, and your and your child’s consent sought in the normal way.
Please stay on the ward during the procedure in case something comes up and we need to speak to you straight away.
I will come and speak with you as soon as I can once the procedure is finished, and your child will be observed by a nurse. Tell the nurse if your child has any symptoms such as chest pain or difficulty breathing. The nurse will check the blood pressure, pulse, respiratory rate and oxygen saturation. Your child cannot eat or drink anything for 1-2 hours after the procedure because the throat may still be numb.
Many children stay overnight as other procedures are being carried out; I also get infants to stay as an extra precaution. However for those going home the same day, once your child has eaten and drunk and is comfortable, you will be able to leave, assuming the nurse is happy with the blood pressure etc.
If you are concerned about your child after you have gone home, you can always speak to a doctor. Please ring the hospital (0207 352 8121) and ask the operator to bleep the on-call paediatric respiratory registrar.
There are always small risks in having an anaesthetic, and the anaesthetist will explain these to you. There are also small risks in having a bronchoscopy. However, we perform more than 200 of these on children every year at this hospital, and the vast majority of these are without complications. The commonest reaction is a slightly high temperature, and normally paracetamol (Calpol) deals with this. Some children cough a bit more for the next 12-24 hours. We also caution parents of babies having the procedure in order to investigate stridor (noisy breathing due to difficulty breathing in) that they may need extra monitoring, or help with their breathing for a while afterwards. If necessary, they will be cared for in the paediatric intensive care unit, or high dependency unit and the anesthetist makes that decision at the end of the procedure.
View looking through a bronchoscope. the picture on the left shows the trachea (windpipe) looking down to where it divides into the left and right main bronchi, which are the airways leading to the left and right lungs. The picture on the right is a view of the airways in the left lower lobe